
Boosting NICU Safety
How pharmacist interventions reduce drug-related problems in newborns
Norhan Attia, Clinical Pharmacist, Assiut University Hospital
Neonates in NICUs face heightened risks of drug-related problems (DRPs) due to complex treatments and physiological immaturity. A study at Assiut University, Egypt, found DRPs in 89.6 per cent of neonates, primarily stemming from treatment effectiveness problems. Clinical pharmacists achieved a 92 per cent resolution rate, highlighting their critical role in enhancing neonatal care.
Introduction
Neonate is a ''child under 28 days of age'' [2]. In the Neonatal Intensive Care Unit (NICU), neonates are particularly vulnerable to drug-related problems (DRPs) due to several factors, including their critical condition, the complexity of their treatment regimens, the immaturity of their physiology, and the challenges of multidisciplinary care [3]. As defined by Pharmaceutical Care Network of Europe (PCNE) classification, Drug-related problems are described as "an event or circumstance involving drug therapy that actually or potentially interferes with desired health outcomes". It is important to note that drug-related problems are an umbrella term that encompasses medication errors, adverse drug reactions, and adverse drug events, which are often mistakenly used interchangeably with DRPs. This comprehensive understanding of DRPs underscores the unique vulnerability of neonates in the Neonatal Intensive Care Unit (NICU) and highlights the importance of addressing these issues to improve health outcomes. The prevention of patient harm starts with the identification and categorisation of potential DRPs by pharmaceutical services [4]. The World Health Organization (WHO) recognises pharmacists as vital resources for the efficient and safe administration of medications [5]. Their role is crucial in ensuring the accurate dosing, monitoring for potential drug interactions, and providing essential recommendations to the healthcare team, thereby enhancing the safety and efficacy of neonatal care.
This is a study conducted over 4 months at Children's University Hospital, Assiut University in Egypt, involving 316 neonates. It aimed to assess the incidence and types of DRPs using the PCNE V9.1 classification and the effectiveness of pharmaceutical interventions in mitigating these risks. This research highlights the critical role of clinical pharmacists in enhancing drug safety and improving patient outcomes in the NICU setting.
Key Findings
Incidence and types of DRPs:
DRPs were identified in 89.6 per cent of the neonates, with a total of 1723 DRPs occurring. Treatment effectiveness problems accounted for 46.4 per cent of these incidents. The main cause of suboptimal treatment was dose selection, accounting for 61.9 per cent of the 2,041causes, with suboptimal doses specifically representing 27.6 per cent (1,264 dose-related causes, including 563 due to doses being too low).
Problems related to effectiveness are common in NICU due to the challenges associated with weight-based calculations, the rapid physiological changes in neonates.
Other problems were miscellaneous problems (27.2 per cent) and treatment safety (26.4 per cent) Figure 1.
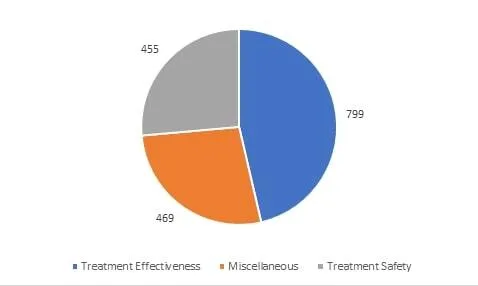
Figure 1 Types of DRPs classified according to PCNE V9.1
According to a French scale adapted from Hatoum et al., 98.7 per cent of these problems were preventable [6].
Pharmaceutical interventions:
Pharmaceutical interventions were primarily focused on optimising doses, resulting in 2149 interventions, with 44 per cent involving dose change.
The acceptance rate of pharmaceutical recommendations by healthcare staff was remarkably high at 98.8 per cent. This underscores the collaborative environment within the NICU and the trust in the clinical pharmacists' expertise. Implementing these interventions led to a 92 per cent resolution of identified DRPs, demonstrating a significant improvement in patient safety and outcomes.
Furthermore, 99.7 per cent of the interventions potentially enhanced the safety and effectiveness of treatment, highlighting the significance of these interventions.
DRPs and Medications:
During the study period, 1888 drugs were prescribed, of which 1726 were involved in DRPs.
The most affected drug groups were anti-infective drugs (64.5 per cent), followed by cardiovascular drugs (11 per cent) and nervous-system drugs (7.2 per cent) Figure 2. Neonates are vulnerable population to infections due to their immaturity and low immunity.
The two anti-infectives drugs most frequently involved in DRPs were amikacin and ampicillin-sulbactam. These agents are particularly challenging, as the dose of ampicillin-sulbactam depends on the ampicillin content, while amikacin, like all aminoglycosides, poses challenges in dosing schedules.
This is particularly relevant as they are frequently prescribed for the treatment of neonatal sepsis
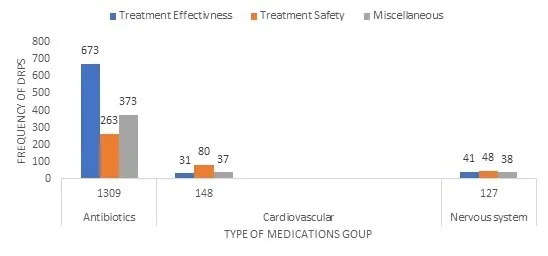
Figure 2 Groups of medications involved in DRPs
Surprisingly, it was found that the medications the least prescribed had the highest risk ratio.
Alprostadil had the highest risk ratio, as this medication requires complex calculations and special considerations to improve safety.
Patient related factors:
It was found that the length of hospital stay and poly-pharmacy pose a significant threat for producing DRPs. The longer a patient stays in the hospital, the more they are exposed to medications. Additionally, more complex cases often require more medications, leading to an increased incidence of drug-related problems.
Discussion:
These findings underscore the indispensable role of clinical pharmacists in the NICU. By implementing pharmaceutical interventions, they significantly enhance drug efficacy and safety, emphasizing the necessity of integrating them into neonatal care teams. Notably, while clinical pharmacy took root in America and Europe in the 1960s and 1970s, its development in Egypt started much later, in the 2000s. The delayed integration in Egypt underscores the ongoing imperative to strengthen this crucial aspect of healthcare.
One of the primary challenges identified was frequent dose errors, particularly suboptimal doses, which significantly contributed to efficacy-related problems. This issue poses a substantial threat to neonates, especially concerning anti-infective drugs, as it heightens the risk of bacterial resistance and treatment failure. Addressing these challenges through targeted pharmaceutical interventions not only improves individual patient outcomes but also bolsters public health efforts by mitigating risks such as bacterial resistance.
Moreover, the remarkably high acceptance rate of pharmaceutical recommendations (98.8 per cent) and the successful resolution of 92 per cent of identified DRPs underscore the profound impact of clinical pharmacists. These professionals play a pivotal role in identifying and rectifying dosing errors, thereby ensuring safe and effective treatment regimens for neonates.
Prolonged hospital stays not only extend medication exposure but also escalate the likelihood of cumulative drug interactions and adverse effects. Vigilant monitoring and regular reassessment of treatment plans are crucial to mitigate potential DRPs arising from extended stays.
Furthermore, the correlation observed between poly-pharmacy and DRPs highlights the intricate nature of medication management in neonatal intensive care. Neonates with multiple comorbidities often require a combination of medications, increasing the risk of prescribing errors, dosing inaccuracies, and adverse drug reactions. Clinical pharmacists are instrumental in optimising medication regimens, ensuring accurate dosing, and minimising DRPs through proactive intervention and close collaboration with the healthcare team.
Clinical Implications:
- Routine Pharmaceutical reviews and interventions should be standard practice in NICUs to minimise DRPs and improve patient outcomes.
- Training programs for healthcare professionals in NICUs should emphasize the importance of pharmaceutical care and equip staff with the necessary skills to identify and address DRPs effectively.
Future Directions:
- Future research should focus on developing standardised protocols for pharmaceutical interventions in the NICU and exploring their cost impact.
- Long-term studies are recommended to assess the sustained impact of these interventions on neonatal health outcomes.
- Expanding the role of clinical pharmacists to include more direct patient care activities and decision-making responsibilities could further enhance the safety and efficacy of neonatal drug therapy.
Conclusion
This study demonstrates that pharmaceutical interventions are highly effective in reducing DRPs in the NICU. These interventions not only improve treatment efficacy and patient safety but are also well-accepted by healthcare providers. Integrating clinical pharmacists into NICU teams is a crucial step towards optimising neonatal care. By systematically identifying and addressing DRPs, clinical pharmacists can significantly reduce the incidence of ADEs, ultimately leading to better health outcomes for neonates. This research underscores the importance of pharmaceutical care in high-risk environments and provides a framework for implementing similar interventions in other critical care settings.
References:
- Ahmed NA, Fouad EA, El-Asheer OM, Ghanem ASM. Pharmaceutical interventions for drug-related problems in the neonatal intensive care unit: incidence, types, and acceptability. Frontiers in Pharmacology. 2024;15.
- Muhe LM. Newborn Health. In 2023 [cited 2024 Jun 17]. p. 43–5. Available from: https://www.who.int/westernpacific/health-topics/newborn-health
- Stavroudis TA, Miller MR, Lehmann CU. Medication errors in neonates. Clinics in perinatology. 2008;35(1):141–61.
- Benson H, Lucas C, Kmet W, Benrimoj SI, Williams K. Pharmacists in general practice: a focus on drug-related problems. International Journal of Clinical Pharmacy. 2018;40:566–72.
- Wiedenmayer K, Summers RS, Mackie CA, Gous AGS, Everard M, Tromp D, Organization WH. Developing pharmacy practice: a focus on patient care: handbook. World Health Organization; 2006.
- Hatoum HT, Hutchinson RA, Witte KW, Newby GP. Evaluation of the Contribution of Clinical Pharmacists: Inpatient Care and Cost Reduction. Drug Intelligence & Clinical Pharmacy [Internet]. 1988 Mar 1;22(3):252–9. Available from: https://doi.org/10.1177/106002808802200318

Norhan Attia, clinical pharmacist with five years' experience at Assiut University Hospital, Egypt, specialising in Neonatal Intensive Care. Expert in medication reviews, IV admixtures, and optimising pharmacotherapy outcomes. Currently a dedicated teaching assistant, focusing on pharmaceutical education and enhancing medication safety in NICU settings.





