
Due to unprecedented economic growth and increased healthcare expenditures, experts predict that by 2012 China will be the world's fourth largest pharmaceutical market. In addition to increased production and distribution by foreign pharmaceuticals, China has become one of the region?s primary locations for outsourcing clinical trials. Growth in the clinical research sector can be attributed to several factors, including China's successful recruitment rates and lower costs. Multi-center trials are most prominent in China, primarily because of the government's promotion of these trials, making them more attractive to foreign sponsors. In addition, the Chinese tend to show a cultural preference for foreign innovator drugs over domestics. Finally, regulatory reforms including the formation of a single regulatory body, the issuing of a Chinese ICH-GCP equivalent, and improved Intellectual Property (IP) protection legislature, have all contributed to China's recent clinical research boom. Despite this, several challenges remain for foreign sponsors, including regulatory hurdles as well as significant linguistic and cultural barriers. These issues will be addressed in the sections below.
Advantages
Patient recruitment statistics demonstrate China?s subject enrolment advantage over most western countries. One study reported that in the United States 66 per cent of subjects in clinical trials enrolled independently of their doctor, while 90 per cent to 100 per cent of participating subjects in China enrolled as a result of their doctor?s recommendation. In China relationships are largely defined by professional position, as well as age and gender. Physicians are therefore highly respected, and patients readily accept their physician?s recommendation to participate in a clinical trial as a course of treatment. Many patients have not received any treatment, making them eligible subjects for clinical research. Moreover, clinical trials offer patients cutting edge treatments that otherwise may not be readily available to them. These factors, along with China?s population of 1.3 billion, greatly facilitate patient enrollment.
The cost of conducting trials in China is significantly lower relative to the west i.e. Chinese salaries are 60-80 per cent less, and clinical costs are 60-70 per cent less per patient. The high level of clinical research produced in the country can be attributed to the abundance of skilled Chinese investigators, many of whom have been educated or have experience working in the west. Most clinical trial sites are located in major urban areas where infrastructure and IT are better established, and in the case of Shanghai, cutting edge. Reportedly 80 per cent of medical resources in China are allocated to major cities, and 30 per cent of this is focused on larger hospitals.
Regulatory environment
China's improved regulatory environment has played a major role in the growth of outsourced clinical trials. The formation of the Chinese State Food and Drug Administration (SFDA) eliminated conflicting standards between provincial government agencies, and resulted in a centralised Chinese healthcare regulatory system with increased transparency. These regulatory reforms, along with a shortened regulatory approval process and the presence of FDA offices in China have all been contributing factors (see Table 1).

Despite improvements in China?s regulatory environment, however, several challenges remain. Approval often takes several months despite efforts to streamline, and the requirement to obtain import and export licenses may further delay trial initiation. Furthermore, because the Chinese GCP equivalent is not identical to ICH-GCP guidelines, clinical trials conducted in China may not fully comply with the ICH-GCP standards. Furthermore, corruption and bureaucracy continue to create hurdles for foreign sponsors.
Another issue in China is that only SFDA-approved sites are authorized to conduct trials. SFDA-accredited sites are unique to China, since prior to the 1970s the country produced primarily generics and initiated few innovative drug studies. However, there are a growing number of approved sites located primarily in large metropolitan hospitals. Finally, foreign sponsors often encounter logistical problems such as the restriction or prohibition of whole blood/DNA export and limited qualified logistic support, for example, central storage, IVRS, fax line, and broadband for EDC.
Language & Translation
Although there are a growing number of advantages for foreign sponsors outsourcing clinical research to China, there are significant linguistic and cultural barriers. As a result, foreign pharmaceutical companies must address linguistic and cultural issues to ensure that they communicate effectively with patients, clinical trial staff, ethics committees, and regulatory authorities.
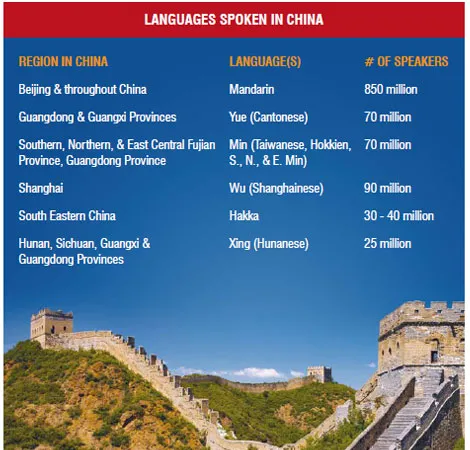
Patient populations in China are diverse. Although the majority of China's population speaks and understands Mandarin Chinese, for a significant portion of people, it is not their first language. Thus, despite the fact that Mandarin Chinese is China's official language (850 million speakers) and the only written form of the language, there are several other dominant languages spoken throughout the country (see Table 2). Among the most dominant are Shanghainese (90 million speakers), Min (70 million speakers), and Cantonese (70 million speakers). Most Chinese languages are mutually unintelligible, and each language has several spoken dialects. Moreover, in addition to the official language based on the Beijing dialect, there are several other regional dialects of Mandarin Chinese. Although for the most part these are mutually intelligible, they must be considered for subtle differences in the meaning of certain words or language use. Finally, to complicate matters further, written Mandarin has two character types. In mainland China, the original Traditional Mandarin characters were changed to Simplified Mandarin characters to help simplify the writing system. However, some minority Chinese populations may still use Traditional Mandarin characters, especially in Taiwan and Hong Kong. Furthermore, depending on the level of literacy, proficiency in written Mandarin varies. In addition, despite English speaking proficiency among the many Chinese-born scientists educated in the west who have returned to work in China, the majority of the Chinese population is not fluent in English or other foreign languages. As a result, foreign companies must use interpreters to help them communicate with clinical trial staff. Thus, language presents a significant communication barrier for western companies working in China, making it essential to employ expert translators and interpreters.
Linguistic Validation & Cultural Adaption
Most study documents must be translated into Mandarin Chinese for submission to the Chinese SFDA and Ethics Committees. Although this single translation requirement simplifies the regulatory process, translation of these documents requires a high degree of accuracy and texts must be culturally adapted for the target audience. Professional translators know the standard terminology, can best identify language equivalents, are familiar with different cultural aspects that must be addressed, and use Translation Memory? which decreases both the time and cost of translation. These experts use an established process to translate clinical trial documents, and are best equipped to overcome any linguistic or cultural barriers.
Over the course of a study several types of patient-related information must commonly be translated. For example, patient questionnaires and patient reported outcomes (PROs) are primarily constructed in English and therefore they must be adapted for Chinese patients. Translating these materials involves linguistic validation and cultural adaptation, an arduous and lengthy process which can take up to several weeks.
The reason for this is that Mandarin Chinese is not closely related to most western European languages or English. Sentence structure is significantly different, isolated phrases or words may have multiple meanings, and some words may be represented by the same characters despite differences in grammatical form. Moreover, written Mandarin Chinese has a unique grammatical structure quite unrelated to that of English or other western European languages from which documents are commonly translated. Thus, translation typically requires a series of forward and back translations, as well as a number of reviews in order to ensure that the intended meaning is accurately and successfully conveyed. Finding the equivalent term and meaning of a phrase or word is not always straightforward, even for experienced translators.
Numerous studies have demonstrated the difficulties encountered in the translation of clinical research documents into Mandarin Chinese, primarily from English. Many of these studies are aimed at creating effective instruments for Chinese patients. They offer insight into the unique challenges related to translating these documents into Mandarin Chinese. Primary examples involve patient reported outcomes (PROs) and Health-Related Quality of Life (HRQoL) patient questionnaires.
One study involving Chinese-speaking patients living in California encountered the following challenges when linguistically validating PROs.
- Since written Mandarin Chinese is composed of characters and not letters, initials or abbreviations are not typically used. In order to identify initials for an abbreviation of a word, translators had to first phonetically translate Chinese names into English.
- In Mandarin Chinese the words for ‘assess’, ‘assessing’, and ‘assessment’ all use the same character, as do ‘treat’, ‘treating’, and ‘treatment’ thus the original English title, “Assessing and Treating Symptoms of Critically Ill ICU Patients” most closely translated into Chinese as “ICU Critically Ill Patients' Symptom Assessment and Treatment”.
- The English term ‘short of breath’ was problematic because in Mandarin Chinese ‘short’ means ‘not long’ and ‘breath’ is not described as short or long. Thus, ‘short of breath’ was changed to ‘hard to breathe’ for Chinese patients.
Another study demonstrated other examples of issues encountered in the process of translating patient questionnaires from English into Mandarin Chinese. The goal of this study was to help define symptom scales for patients in China suffering from various diseases including arthritis, obesity, diabetes and Ankylosing Spondylitis.
Investigators identified the following issues:
- Mandarin Chinese does not use superlatives thus ‘the worst’ had to be translated as ‘extremely bad’ to represent extremes on a scale.
- Chinese patients commonly receive acupuncture and massage therapy, often as a treatment in conjunction with or as an alternative to clinical treatments. These categories had to be added to the questionnaires.
- In Mandarin Chinese questions cannot begin with ‘how often’ and had to be phrased ‘does it often.’ 4. Some patients could not understand the terms ‘full time’ and ‘part time’ and the question had to be phrased ‘Do you work full time (8 hours a day) or not full time?’
A third study, focused on creating a Chinese version of a HRQoL questionnaire for Chinese patients in Hong Kong with spinal deformity, demonstrated the importance of using cultural adaption and linguistic validation in the preparation of such a questionnaire. Scientists in the study noted that the questionnaire was valid only for one particular urban population in China, and that the same version could not be used for other Chinese populations such as those of more rural areas.
Cultural factors
In addition to language barriers, foreign sponsors must have an awareness of important aspects of Chinese culture that affect clinical research. Cultural aspects can inadvertently interfere with both reporting and interpretation of patient data, shape patient perception of disease and symptoms, and determine medical practices. Below are some examples.
Dementia & Alzheimer’s patients in China remain largely undiagnosed and untreated due to the cultural perception that memory loss is part of the aging process. In general, there is a lack of awareness about the relationship of illness and memory loss which leads to delayed treatment in Chinese patients. One study reported that only 21 per cent of patients in China had access to diagnostic assessment compared to over 70 per cent in Europe, largely because Chinese patients did not seek care.
Gender in Chinese society has also been identified as a barrier. One study involving Chinese-American women with cancer found that family decision-making played a major role in a woman’s decision to enroll. Several studies conducted on Chinese immigrants in the United States also identified cultural attitudes among Chinese women that interfered with both preventive care and treatment of Chinese-American breast cancer patients.
Patient reporting of the severity and impact of disease symptoms, an essential component of symptom management and treatment in clinical trials, is significantly affected by cultural attitudes. Symptoms such as pain are often under-reported by Chinese patients. This phenomenon has commonly been observed in cancer studies, along with a less use of analgesics by Chinese patients. These differences in pain perception may lead to the misinterpretation of study results due to inaccuracies in patient data.
Use of traditional natural & herbal therapies by Chinese patients enrolled in a clinical trial may inadvertently affect patient data and study results if they are not reported. Since sponsors are more aware of the extent of this practice in China, this is becoming less of an issue. Additionally, studies are being conducted to determine the effects of such practices on disease, symptoms, and conventional therapies.
Conclusions & recommendations
Recent economic growth, along with China’s growing potential drug market, has played a pivotal role in the increase in foreign-sponsored clinical research. China offers several advantages over western countries, including a large diverse primarily treatment naïve patient population and significantly reduced costs. With recent improvements in regulatory procedures, an influx of Chinese-born scientists educated in the west, and changing disease trends, there is an even greater incentive to conduct clinical research in the country.
Despite the advantages, several challenges remain including significant linguistic and cultural barriers. However, if these issues are properly addressed they can be overcome. Translation experts familiar with working in China are best equipped to deal with the challenges of preparing regulatory documents in Mandarin Chinese. Studies involving linguistic validation and cultural adaptation of patient questionnaires and PROs further emphasize the importance of using a well established process. Finally, aspects of Chinese culture that affect patient reporting, enrollment, and medical practices must also be considered when conducting clinical studies in China.
Disease Trends
Clinical research in China encompasses a wide range of therapeutic areas, including respiratory and cardiovascular diseases, as well as diabetes, obesity, and cancer. The incidence of cancer is growing as a result of population aging and growth as well as an adoption of cancer-associated lifestyles including smoking, physical inactivity, and ??westernized?? diets. Breast cancer is the primary cause of death in Chinese women largely due to inadequate prevention and detection during early stages. Chinese women also tend to have higher lung cancer rates than women in more developed western countries as a result of exposure to toxins. The rate of lung cancer rates in Chinese men is also rising due to an increase in smoking. According to recent statistics, China currently has the largest diabetes patient population in the world, having recently overtaken India for first place.





