
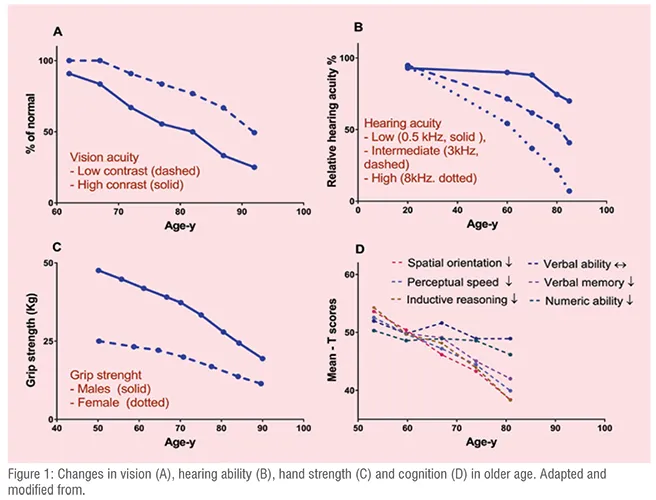
There is a rising opportunity for the pharma industry to consider developing products and administration devices for older age population. The proportion of the elderly population is growing globally. Age associated comorbidities has resulted in larger need for medication use and appropriate delivery systems. The older age population are extremely heterogeneous, each individual has their own specific needs. The physiological functions varies among the individuals, this depends on ethnicity, genetics, social interaction and life style etc. Generally, the drug delivery systems are being developed more from a technical perspective with the focus to provide more easy, timely and targeted delivery. However, for older person, especially those who suffer from vision impairment, hearing loss, cognitive impairments, the delivery systems that are easy to use, allowing self-administration, is of importance. As shown in the figure 1 there is age related decline in important senses and functions in older persons that can impact on the proper drug administration and can also impact on adherence. Adherence is a key marker for the efficacy of the medications and is an important factor to be consider in the development of drug administration devices. It is suggested that the administration device, the product safety, including both active and non-active ingredients, packaging/labelling and product information that are suitable as per older person needs and capabilities are required for optimum therapeutic outcome.
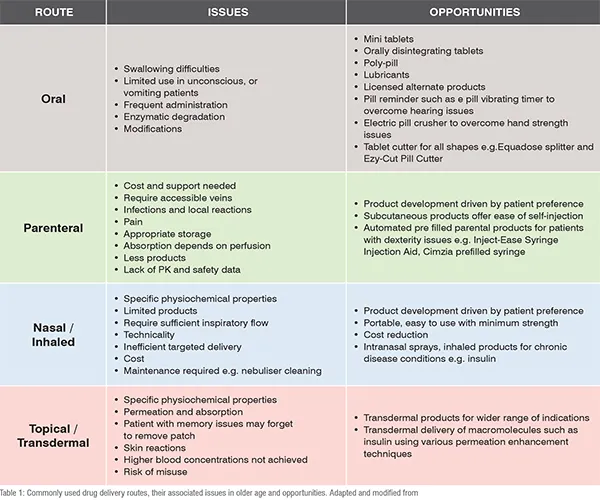
The pharma industries are encouraged to focus on patient-centric product development, distinctive from technological driven products. In particular, older person taking large number of medications require assistance in identifying their products and need reminders to take the products timely. Non adherence can be an issue for older patients on polypharmacy, comorbidities, and in patients having dexterity issues, visual impairments, cognitive problems and functional disabilities. Almost 50 per cent of patients suffering from chronic diseases are unable to take their medications as directed. Single unit dose packaging, clear labelling, easily opened products will allow self – administration, will reduce dosing errors and will minimise the wastage and contamination. Product information with large fonts and high contrast imprints will benefit elderly with poor vision in product identification with similar size and shape. Older person with dexterity issue has been shown to benefit from using large triangle shaped screw cap, instead of rounded cap for opening the bottle. Including calendars and other aids within the drug delivery systems will improve adherence and minimise risk that are associated with missing and doubling the dose. Commonly used administration routes, related issues in older age and needs for innovation is shown in table1 and will be discussed as follows.
Oral Drug Delivery and Older Age
Swallowing issues are most common with oral dosage forms such as tablets and capsules in older persons. Large size tables can easily stuck in the oesophagus. Patients are also hesitant to swallow large tablets, in particular those having condition known as dysphagia (a medical condition describing swallowing difficulty). These patients often require crushing their tablets. As example, in nursing home mixing crushed medications with food is a common practice. Some products such as enteric coated tablets cannot be crushed. The size, shape, taste issues can also make patients hesitant to swallow solid oral dosage forms. Developing technologies that facilitate ease of swallowing are required. As example, some of the recent developments include disposable coating devices, where a thin coat of flavour is applied via a spray. This practice was found useful in elderly patients with swallowing difficulties. For powders or liquids premeasured sticks termed as stick-packs were found useful. These are single dose package that can be filled with either liquid or powder. In older patients with tremors, studies have shown that dosing errors was reduced with the use of liquid stick packs. Some conditions such as neurogenic oropharyngeal dysphagia reduces sip size, therefore further developments in these technologies are needed.
The concept of using a polypill, where the products are combined together to produce a single tablet is also promising and reduces the pill burden in older person taking multiple medications. Polypill was found cost effective intervention in elderly population and can improve therapeutic outcomes. The challenges with the use of polypill technology is the compatibility of the dosing schedule of different products as well as tablet size can be difficult to swallow. Having knowledge of older person preferences, their needs, habits, treatment duration is important to identify best route, drug and suitable technology development. In the early phase of drug delivery system development, feedback from elderly patients and care givers can be beneficial to improve outcomes.
Dosage form modifications are often required in older persons, however the unavailability of licensed dosage forms results in higher cost. An example of such kind is unlicensed quetiapine suspension which was found 10 times more costly than quetiapine tablets. The opportunity to develop alternate licensed products that meets older person’s needs can be of commercial value. An example is the development of riluzole suspension formulation. The oral dosage form of this product was difficult to swallow by almost 80 per cent of the patients. The product was crushed but it was found to have oral anaesthetic effects on the tongue. Another innovation is to include lubricants in solid dosage forms such
as Gloup. These can overcome the disadvantages associated with using thickeners which can sometime impact on drug dissolution. In general, viscosity of 150 mPa.s and above impedes drug release. In the absence of alternative dosage forms, a scored tablet can be used to cut tablet in to two pieces, however caution is required as studies have shown the variation in doses of up to 3 fold. Mini tablets have also shown to improve acceptability in older age patients. Older patients found it easy to swallow tablets with a diameter of 3 mm or less.
Some dosage forms such as Orally Disintegrating Tablets (ODTs) dissolves in the mouth and is then swallowed. ODTs has shown higher preference in patients with dysphagia, migraine, and other CNS disease with rapid onset of actions. In older person, reduce saliva production can affect its use. As example, sublingual Nitroglycerin tablets has shown slower absorption rate in the older patients then younger patients. Taste, packaging and specialised equipment’s are important consideration for ODTs manufacturing. Multiparticulate controlled release formulations are also rapidly evolving and can be advantageous for older people as they can be compacted to mini-tablets and packed to sachets, however excipients safety can be of concern.
Nasal Drug Delivery Systems and Older Age
Intranasal route has advantage of easy access, fast onset of action and ease of use. This route is currently being investigated for delivering medicines for both local and systemic use. The potential candidate drugs are opioids, respiratory drugs, vaccines and anti-diabetic drugs. As example, Butorphanol intranasal product was found as effective and safe as IV product in older patients. The bioavailability of certain drugs were also found upto 3 fold higher with nasal sprays compared to nasal drops. However there are limited intranasal products available due to specific requirements of lipophilicity, molecular weight etc.
Pulmonary Drug Delivery and Older Age
Pulmonary delivered drugs are absorbed by alveoli of lungs. Alveoli has rich blood supply and large surface area, which ensures high availability of both small and large molecular drugs. However, a range of challenges remain with this route such as development of higher anti-insulin antibodies. The treatment of conditions such as asthma and Chronic Obstructive Pulmonary Disease (COPD) through these routes is well established. The key challenges associated with this route are age related reduction in lung functions, dexterity issues, patient suffering from arthritis and cognitive issues. These issues can result in altered pharmacokinetic and pharmacodynamic of drugs, ineffective inhaler technique and poor outcomes. Studies have shown that almost 40 per cent of the older patients aged 80 years failed to use an inhaler.
Common inhaler devices that are in use are pressurised Metered-Dose Inhalers (pMDIs) with or without spacer, Dry Powder Inhalers (DPIs) and nebulisers. Patient education through instruction and demonstrations has played an important role in appropriate use of these devices. The issues with pMDIs in older people are inability of activation by breath, hand strength requirement, cost of spacer and portability of device. DPIs need certain inspiratory flow and appropriate storage. Nebulisers can be use in elderly with poor strength and cognition but requires support and can be toxic in case of droplets escape. Some products such as Soft Mist Inhalers (SMIs) Respimat® Soft Mist™ Inhaler is a good example developed to overcome issue with existing devices. The device overcomes the need of hand-breath coordination and inspiratory flow that is required for some other devices and is without propellants, however cost is an issue. Newer products, Smartinhaler™ has remote usage monitoring and dose reminder technology. However, issues are technical complexity and cost. In general studies have shown preferences for inhaler considering size, number of steps, comfort of mouthpiece and opening and once daily dosing. Pulmonary drug delivery in older age can be a promising alternative as compared to invasive delivery systems. Afrezza (human insulin) inhalation (Mannkind, FDA approved in 2014), is an alternative non-invasive insulin delivery systems to self-injected insulin.
Transdermal Drug Delivery Systems and Older Age
The advantage with transdermal system is improved adherence and minimising the drug dosing frequency. Oxytrol transdermal patches, used for urinary incontinence, are used twice weekly and are readily available over the counter. Another potential utilisation of transdermal products are in older patients with neurological problems. Rivastigmine and rotigotine transdermal patches avoid swallowing issues and multiple daily dosing in Parkinson’s disease. Some products may be associated with adverse events, for instance light headness and dizziness were found with transdermal fentanyl use in cancer pain patients. Age related changes in skin physiology, cognition can affect the use of transdermal products. The patients may forget to remove their patches and can be exposed to overdoses. Older people may get skin irritation and allergies with the use of transdermal patches. The nature of the drug for development as a transdermal product is an important consideration. The potential drug candidates are highly potent, having small molecular weight (MW<500 Da), lipophilic, Log P of 1 to 3 and are uncharged.
Pharmacokinetic and Pharmacodynamic Considerations in Elderly
Pharmacokinetic (PK) is defined as what body does to the drug and Pharmacodynamics (PD) are the physiological effects of the drugs. PK include four important processes namely absorption, distribution, metabolism and excretion. Important body function that are most relevant to impact on PK of the drugs are changes in body composition, small intestine surface area, gastric emptying, liver function, kidney function and changes in blood flow to these important organs etc. A thorough understanding of the physiological changes with ageing is important to understand the impact on PK of the drugs, these changes are presented in details in our recent articles. Medications use need caution in elderly due to age related alterations in PK. In general drug distribution can be affected by the changes in body composition such as increase in body fat can prolong half-life and exposure to the drugs such as diazepam. Reduction in liver function such as reduced size, less blood supply can decrease clearance and can expose elderly to higher drug levels. As example, the clearance of lithium is reduced in elderly. From PD perspective, older people may have increased sensitivity to some drugs such as benzodiazepines and opioids.
A large body of work has already been performed in previous years to address ageing effects on PK of drugs. However there are still limited data in patients with very older age, frail and patients with comorbidities and polypharmacy. The current focus in drug development is to undertake studies in healthy subjects, excluding patients with confounding factors such as decreased kidney functions, frail and with multiple medications. The data obtained from these studies may not be applicable in actual clinical practice, especially in older frail patients with polypharmacy. Limited data is also available for newer drugs coming to the market such as novel oral anticoagulants and anti-diabetic drugs that are commonly used for the management of chronic disease conditions. In addition PK data is also needed in increasing very older population group 80 years old and above. Supporting and conducting clinical studies in more realistic environment involving older patients with varying degree of organ functions, frailty status, polypharmacy can help in generating data that can be applied to clinical practice in real world. The data from these studies can be used to develop physiological based pharmacokinetic models which can then be utilise to predict pharmacokinetic parameters of drug products in older people. Collaborations between industry and academia are key to successful advance in this area.
The Issue of Polypharmacy in Older Age
As the age increases the medication use also increases. Upto 88 per cent of the older person use at least one prescription medicine. Polypharmacy, generally defined as the use of five or more regular medications is prevalent in almost 40 per cent of the older adults. Among older hospitalised patients with a mean age of 81 years almost half of the patients used 5 to 9 medications and 30 per cent of the patients used 10 or more medications, often referred to as hyperpolypharmacy. Older persons living in nursing homes, on an average use 14 (±4.7) medications. The risk of potential drug interactions increases with polypharmacy and can cause serious adverse events and geriatric syndromes such as falls, delirium, cognitive issues and depression. The use of herbal medicines is generally not recorded in routine practice which has also increased over the years among older persons. In one survey of population above 75 years, almost one third of the patients were using one dietary supplements together with prescription medicines. Interactions of herbal medicines with prescribed medicines can lead to adverse events. For instance, ginkgo biloba extract can interact with warfarin and increase bleeding risk. Similarly in older adults, St. John's wort can increase the risk of serotonin symptoms when taken with serotonin-reuptake inhibitors. Pharmaceutical industry can play role in supporting patient education which include relevant and easy to understand information about products, drug-drug interactions and drug disease interaction and expected side effects. There can also be a potential role for pharmaceutical industry in promoting health carer education for older patient care.
Conclusion
Older age population is currently 9 per cent of the total global population, but are the largest consumers of prescription and over the counter medicines. Their population is on rise and will reach to 28 per cent of total population in particular regions of the world by 2050. The following recommendation can be considered
- Developing useful alternative products in patients with issues such as swallowing difficulties
- Develop safety guidelines and information for medicine modification, crushing or mixing with food
- Developing delivery systems or administration aids that can be used in elderly with independent living and with varying functional capabilities and senses
- Developingpoly-pill or fixed dose combinations product to reduce pill burden on elderly
- Involving patients and their career in the early phase of drug delivery systems e.g. devices used in inhaled products
- Promoting research and collaboration between industry and academia.
Acknowledgements and Disclosures
Michael Roberts would like to acknowledge the support by grants from the National Health and Medical Research Council of Australia (1107356 and APP1055176) and the US FDA grants (U01FD005226 and 1U01FD005232-01). Muhammad Suleman Khan would like to acknowledge the support by post-graduate research scholarship from University of Queensland and support from NHMRC Translational Australian Clinical Toxicology (TACT) Program Grant. No conflicts of interest to be declared.
Keywords:
Older age, frailty, drug delivery systems, pharmacokinetics, polypharmacy, comorbidity, adherence, innovation.
Terms used:
Comorbidity: The existence of one or more additional condition/conditions co-occurring with a primary condition. E.g. hypertension with diabetes
Dysphagia: A medical condition describing swallowing difficulty
Frailty: A geriatric syndrome characterised by reduction in physical and cognitive reserves that leads to increased weakness
Polypharmacy: Generally defined as use of five or more regular medications Pharmacokinetics: Movement of the drug in the body






